
“Your involvement in his care was overstated”
I read that text from the ICU attending and realized, yes, all I did for this patient was close his abdomen. Out of all his doctors, I was probably the least important. He was battling cancer and had multiple treatments, complex surgeries, and several doctors before I met him. The first time I met him was while he was asleep in the OR with an open abdomen. Yet, why did I care so much and why was I so insistent on having the ICU team update me on his status?
During my plastic surgery training, I started rounding by myself in the evening without other residents or students. I would sit down with the patients and talk with them. Talking one-on-one instead of in the usual large medical rounding entourage made the patients more comfortable telling more personal details about themselves. I learned about them, their stories, their families, and their hopes, dreams, and fears. It didn’t take much – just an extra 15 minutes of my time, but it became something that made a big difference. Because I knew my patients better, I could pick up changes in their condition sooner. Because they were comfortable with me, they spoke up sooner. Their families weren’t afraid to tell me subtle changes in their loved one’s condition. For me, I had a good time meeting and talking with the patients and it re-energized me. It was my way of keeping me grounded and centered.
I continued solo rounding when I became an attending. No matter what was happening with medical school or hospital politics, administration, difficult personalities or policies, I could recenter myself by reminding myself of the reason I was in medicine. As a reconstructive plastic surgeon, my goal is to get the patients back to the life that they want to lead. I listened to their stories about their family, home, pets and I could imagine them back home.
I did my usual solo rounding on this patient during his extended hospital stay. We talked about all sorts of topics. He surprised me with his depth of thought and ability to see different situations from multiple perspectives. During his hospitalization, I explained options of treatment and he was able to understand them completely and relate them to his field of work which wasn’t medicine. He made me smile and laugh. I enjoyed visiting with him, especially as he recovered and his true personality came out.
The last time I saw him awake, he had made it to the rehab facility. I walked in and he started grinning widely. We talked and joked and laughed. Before I left, he told me “I hope I see you again soon” and I said, “You will.”
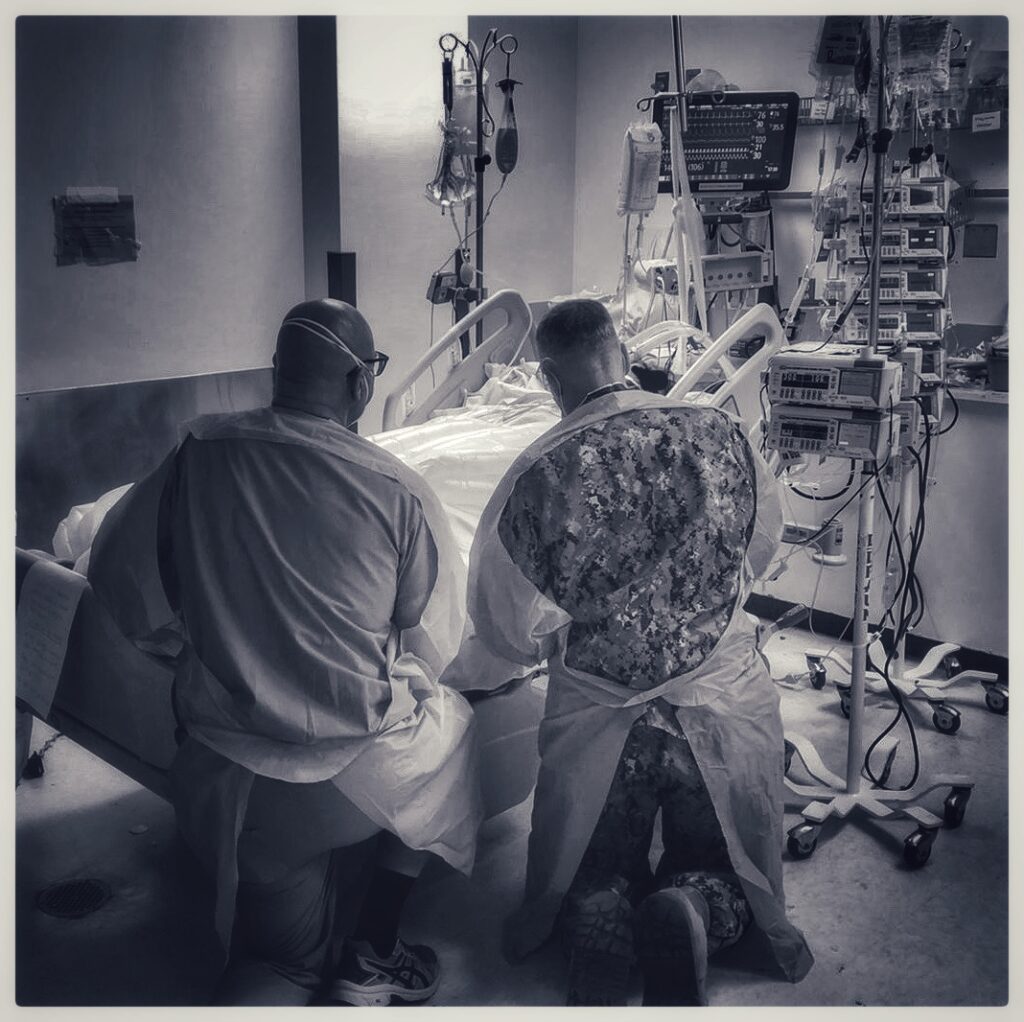
The next time I saw him was in the ICU a day and a half later. He was on multiple pressors, had a tracheostomy, chest tubes, and a brand new stent covering an ileal-iliac fistula. He had coded twice and had undergone massive transfusion protocol due to the blood loss from the fistula. I broke down outside his room, then got myself together, went into the room, grabbed his hand, and said a prayer. I went to his wife and gave her a big hug. Before I left for the night, I insisted that the ICU team give me updates.
The next evening I was out of town for a wedding and I got a text from the ICU attending saying they were going to do an exploratory laparotomy on him. I asked if they needed any information from me and said that all I had done was a Saturday morning abdominal wall reconstruction intraoperative consult. The ICU attending said, “Your involvement in his care was overstated”. I replied “I’m kinda attached to this patient. I like him a lot”. The ICU attending wrote back, “Got it. I’ll keep you informed.”
A few hours later I got a message. The laparotomy was negative, there was nothing else to do and he was going to be placed on comfort care. “Is he going to make it through the night?” I asked. “I don’t think so,” was the reply.
I was in the middle of a wedding reception and over an hour away from the hospital. I told my husband that I had to go see my patient and his family so I hitched a ride back with friends.
I rushed into the hospital and after a quick update from the ICU attending, I went into the room. I walked in the room, gave his wife a big hug and she said “I knew you would come… He was so excited to see you…You are his angel.”
As a plastic surgeon, I don’t deal with death often. This was the first patient of mine that died since I became an attending. I love to make people happy and my goal is for them to leave the hospital better than they came in. I like seeing them in my clinic so I can hear about their home, family, trips and whatever else makes them who they are.
I wonder if I get too emotionally involved with my patients. Some people would say that I do. But, I also realize that if I don’t have this emotional connection with patients, I may lose what drives me to do what I do.
So, I’ll continue solo rounding. I’ll continue going back to the bedside at the end of the day, pulling up a chair, and making the connections that give my job meaning.
Learn more about the ACGME Back to Bedside Initiative
Follow Dr. Shah on Instagram
“It was very difficult to see. The most difficult to see was everybody dying without their familes at their bedside”
Photo by: Dr. Scott Farber